Bridging the gap: First-cycle results of a multi-centre NHS survey on junior doctors’ confidence in managing acute orthopaedic emergencies
By Hatem Husseina, Ahmed Shalaanb, Mohamed El-Gamalc, Mohamed Wahbd and Mohamed Hasheme
aSenior Clinical Fellow, Trauma and Orthopaedics, Southend University Hospital, Mid and South Essex NHS Foundation Trust
bSenior Clinical Fellow, Trauma and Orthopaedics, Bedfordshire Hospitals NHS Foundation Trust
cClinical Fellow, Trauma and Orthopaedics, Southend University Hospital, Mid and South Essex NHS Foundation Trust
dJunior Clinical Fellow, Trauma and Orthopaedics, Wexham Park Hospital, Frimley Health NHS Foundation Trust
eTrauma and Orthopaedic Consultant, Frimley Health NHS Trust
Introduction
Acute surgical and orthopaedic emergencies represent critical time-sensitive scenarios where delays in diagnosis or management can lead to permanent disability, limb loss, or death. Within the NHS, junior doctors, particularly resident doctors at the SHO and core surgical trainee levels, often act as the first point of contact for these emergencies. However, several studies have highlighted a persistent lack of confidence in recognising and managing high-stakes conditions among this group1-3.
This confidence gap continues despite the presence of structured postgraduate training, reflecting disparities in clinical exposure, teaching quality across trusts, and the inherent challenges in managing rare but high-risk pathologies.
Our multi-centre survey across ten NHS trusts assessed resident doctors’ competence in managing six critical orthopaedic emergencies. Each case was evaluated through three domains: documentation, acute diagnosis, and acute management. The selected emergencies were cauda equina syndrome, fractures with neurovascular compromise, necrotising fasciitis, compartment syndrome, spinal cord injuries, and septic arthritis, which represent time-critical scenarios that demand prompt, confident action.
Cauda equina syndrome (CES) represents one of the most time-critical neurosurgical emergencies in the NHS. Studies indicate that earlier surgical intervention is associated with better neurological outcomes, particularly in cases with acute neurological compromise4. In the UK, the incidence of CES is estimated at approximately 1.9 per 100,000 population per year, translating to around 600–1,000 cases annually5. Junior doctors frequently encounter diagnostic uncertainty when faced with subtle or early presentations. Our study specifically examines confidence gaps in red flag recognition and the impact of structured decision aids on referral accuracy.
Fractures with neurovascular compromise present unique challenges in the UK's trauma pathways. While major limb fractures represent about 7% of the patients with upper and lower limb and pelvic fractures admitted to the trauma room. Overall survival was 80% in pelvic fracture and 97% in extremity fracture patients, and comparable to non-vascular trauma patients6. The incidence of major lower limb fractures is about 215.9 fractures per 100,000 patients per year7. The BOASt guidelines mandate that vascular and neurological status should be assessed and documented immediately upon presentation, and this assessment should be repeated systematically, particularly after any reduction manoeuvres or the application of splints8. Our intervention incorporates vascular assessment simulations using pulsatile limb models to address these skills deficits.
Necrotising fasciitis is a rapidly progressive, life-threatening, severe soft tissue infection, which makes early recognition imperative. The age-standardised mortality rate is about 16%, especially with diabetes, old age, chronic renal disease, and heart failure9. Diagnostic challenges are profound, even when using the LRINEC score to guide diagnosis, as with an LRINEC cut-off score ≥6, the sensitivity was 43%, specificity was 83%. In addition, when the LRINEC cut-off score ≥8, the sensitivity was 27% (95% confidence interval 19% to 37%), specificity was 93% (95% confidence interval 91% to 94%)10. We evaluate the efficacy of a novel 'SKIN-SAVE' mnemonic (systemic signs, crepitus, induration, necrosis, speedy progression, abscess mimic, violaceous changes, elevated markers) in improving diagnostic accuracy.
Compartment syndrome demonstrates significant practice variation across NHS trusts. The incidence of acute compartment syndrome is estimated to be 7.3 per 100,000 in males and 0.7 per 100,000 in females, with many cases occurring after trauma11. With early intervention is mandatory to improve the results; still, vague early sign poses a challenge to junior residents, as still no scoring system or definitive scan that is diagnostic. Our intervention introduces mandatory 'compartment checks' using standardised pain assessment tools and timed escalation protocols.
Spinal cord injuries are life-changing injuries with a profound impact on those who are injured and their families. In the UK, there are around 16 new cases per million population of traumatic spinal cord injury each year12. The NICE NG41 guidelines stress that the imaging should be performed urgently and interpreted immediately. Additionally, it recommends a four-hour time frame after the diagnosis to contact the linked specialised spinal injury centre, and the transfer is to be as soon as possible13. Yet we found that most of the residents struggle with spinal clearance, acute management, clear documentation, and imaging interpretation. We assess the impact of immersive VR simulations replicating real-world trauma scenarios on diagnostic confidence.
Septic arthritis is a medical emergency that can lead to rapid joint destruction, reduced mobility, sepsis, and increased mortality, particularly with delayed diagnosis and treatment14. The incidence of septic arthritis in the UK has been increasing over recent years. A population-based study analysing data from 1998 to 2013 reported a rise in incidence from 5.5 to 7.8 cases per 100,000 person-years, representing a 43% increase over the 15 years15. The increase was most pronounced in individuals over 75 years of age, with incidence rates reaching 31 per 100,000 person-years in this age group16. In our study, we assessed the familiarity of the residents with the clinical picture, various investigations, and acute management.
Study aim
This study represents the first comprehensive evaluation of NHS junior doctors' preparedness across these five Trauma & Orthopaedic high-risk emergencies. By correlating confidence levels with objective knowledge assessments and clinical simulation performance, we aim to identify any critical gaps in current training paradigms. Our phased educational intervention, combining structured decision aids, high-fidelity simulations, and trust-specific escalation protocols, aims to standardise competence in managing these time-critical conditions across diverse NHS settings.
Methods
Objectives:
- Assess the baseline confidence of junior doctors in diagnosing and managing five acute surgical emergencies.
- Identify gaps in training and guideline awareness.
- Design and implement targeted interventions to improve confidence.
- Evaluate the impact of interventions via post-survey analysis.
Design:
Multi-centre NHS observational interventional study planned in two cycles, pre-intervention and post-intervention, over a year.
Participants:
Junior doctors managing these emergency cases at 10 NHS Trusts across the UK.
Phase 1 (pre-intervention):
- Surveyed junior doctors across participating NHS Trusts.
- Questions assessed the diagnostic confidence, management confidence, and documentation across the six conditions.
- Collected data from FY1, FY2, SHO, and registrars.
Intervention:
Develop based on pre-intervention survey findings and includes:
- Interactive teaching sessions, incorporating simulation and video-assisted reflection (VAR) training
- Visual display of guidelines and policy posters (NICE and local trust protocols)
- Standardised documentation templates, safety checklists, and easy-to-use diagnostic mnemonics
Phase 2 (post-intervention):
- Re-administered identical surveys to assess improvements.
- Collected feedback on intervention effectiveness.
Inclusion criteria:
- Resident doctors involved in acute surgical or trauma care (SHOs, Registrars).
- LED/Trainee Doctors working in an NHS setting in the UK.
- Consent to participate and submit responses.
Exclusion criteria:
- Consultants and associate specialists.
- Doctors who are not involved in managing the conditions being studied.
- Non-English speakers
- Locum/Bank doctors
Data analysis:
- Surveys were analysed using descriptive statistics.
- Confidence levels were compared across roles for each condition.
- Focus was placed on the three main domains: confidence in Assessment, management, and documentation.
Results
Pre-intervention findings (January–March 2025)
A total of 204 junior doctors across 10 NHS Trusts participated in the pre-intervention survey. Amongst which, 17 FY1, 25 FY2, 103 Junior Clinical Fellow (SHO), 59 Registrars/Middle grades. This survey sought to evaluate the confidence and competence of trainees in managing six acute orthopaedic emergencies. A total of thirty questions aimed to explore three main domains for each condition: confidence in diagnosis and management, and documentation proficiency.
Cauda equina syndrome (CES) emerged as a critical area of concern, particularly among junior trainees. Among the 145 FY1s, FY2s, and SHOs, only 20 individuals (13.8%) could accurately list all the red flag criteria essential for CES diagnosis, a startling statistic given the urgency and medico-legal weight of the condition. Their average confidence score in managing CES was 2.67/5 (53.4%), suggesting significant uncertainty in initiating appropriate steps. Conversely, registrars reported substantially higher management confidence levels, with an average score of 4.3/5 (86%). Interestingly, documentation proficiency was paradoxically better among juniors 3.0/5 (60%) than registrars 2.0/5 (40%), possibly reflecting a cautious approach by juniors despite their diagnostic uncertainty. This is further contextualised by diagnostic confidence scores, where registrars rated themselves at 4.0/5 (80%) compared to 2.8/5 (56%) for junior colleagues, a 24% gap in foundational awareness (Figure 1).
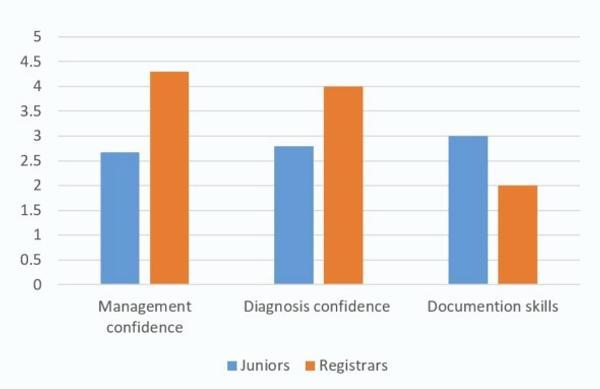
Figure 1: Cauda equine syndrome
Fractures with neurovascular deficit: The contrast between training grades was greater with this clinical scenario. Registrars demonstrated a high level of competence, scoring 4.5/5 (90%) for management confidence and 4.3/5 (86%) in diagnostic confidence. In contrast, junior doctors reported critically low confidence in this domain. Their management confidence with neurovascular compromise was rated at just 1.1/5 (22%), and diagnostic confidence at 2.1/5 (42%). Both figures underscore an urgent need for targeted education. Documentation standards followed the same pattern: juniors scored 2.0/5 (40%) while registrars scored twice as high (4.0/5, 80%). These results suggest that many juniors may not fully appreciate the urgency or complexity of such injuries, leading to delayed recognition and suboptimal early management (Figure 2).
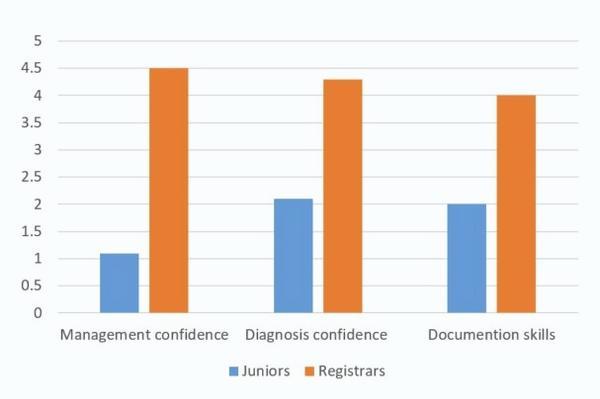
Figure 2: Fractures with neurovascular deficit
Necrotising fasciitis is a rapidly progressive soft tissue infection with high morbidity and mortality, which is also poorly understood among juniors. Their average diagnostic confidence was 2.7/5 (54%), and management confidence was just 2.3/5 (46%). In contrast, registrars demonstrated greater awareness and competence, with diagnostic confidence and management confidence scores of 3.5/5 (70%) and 3.8/5 (76%), respectively. These findings, though expected given the rarity of the condition, highlight a potential risk: juniors may misattribute early signs of necrotising fasciitis to benign soft tissue infections. Documentation again reflected this trend, with juniors at 2.3/5 (46%) and registrars at 4.0/5 (80%), suggesting a consistent gap not only in knowledge but in clinical recording (Figure 3).
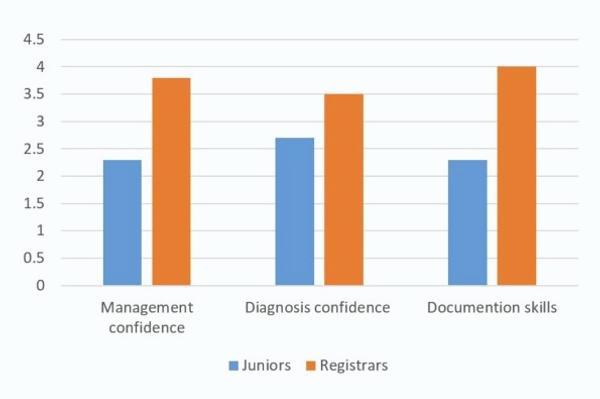
Figure 3: Necrotising fasciitis
Compartment syndrome: With this limb-threatening emergency, the data again underscored disparity. Junior doctors reported a management confidence of only 2.3/5 (46%), while registrars averaged 3.4/5 (68%); a 22% gap. Encouragingly, juniors showed better diagnostic confidence in this condition compared to others, scoring 3.6/5 (72%) versus 4.2/5 (84%) for registrars. This may reflect improved undergraduate emphasis on this diagnosis or increased exposure in trauma settings. Documentation quality was notably higher among both groups, with juniors scoring 3.5/5 (70%) and registrars 4.2/5 (84%), suggesting that once suspicion is raised, record-keeping tends to be more thorough (Figure 4).
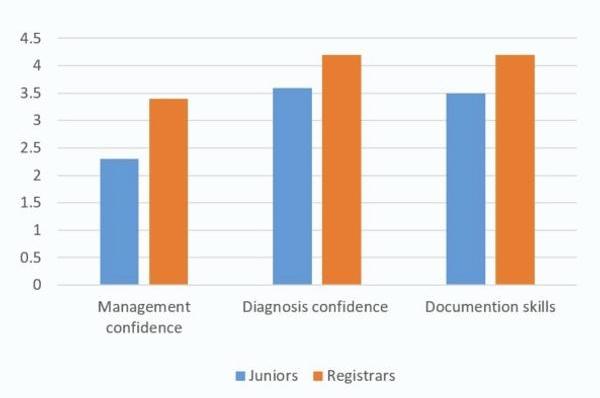
Figure 4: Compartment syndrome
Spinal injuries: In this clinical domain registrars again outperformed junior doctors. They reported an average diagnostic confidence score of 3.8/5 (76%), compared to 3.0/5 (60%) among juniors, signifying a minimum 16% deficit in confidence with spinal assessment frameworks. Management confidence among juniors was 2.8/5 (56%), while registrars rated themselves at 3.4/5 (68%). Though the overall confidence gap (12%) is narrower than in other conditions, it still reflects substantial room for improvement. Documentation proficiency mirrored this, with juniors scoring 2.5/5 (50%) and registrars 3.5/5 (70%), (Figure 5).
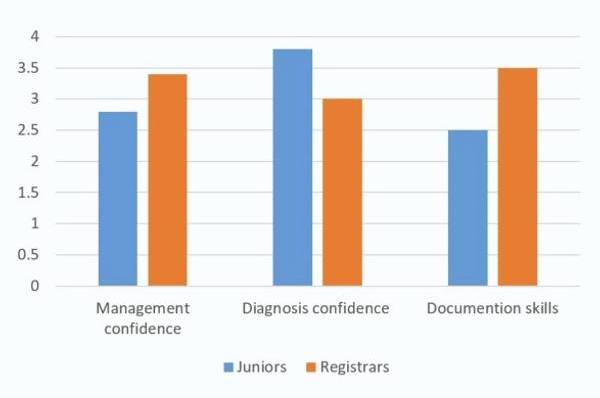
Figure 5: Spinal injuries
Septic arthritis: The condition in which junior doctors showed the highest levels of self-reported confidence. They averaged 3.8/5 (76%) for both management and diagnostic confidence, while registrars reported 4.7/5 (94%) for diagnostic confidence and 4.4/5 (88%) for management confidence. Still higher but with a comparatively narrower gap. Documentation scores were similarly reassuring, with juniors averaging 4.0/5 (80%) and registrars 4.2/5 (84%). These figures may indicate that septic arthritis is more regularly encountered or better taught at junior levels compared to other conditions (Figure 6).
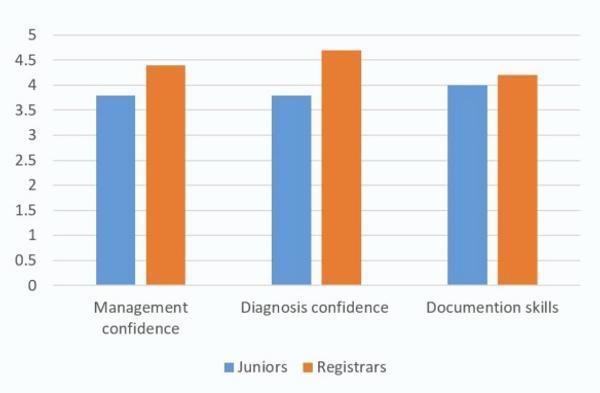
Figure 6: Septic arthritis
Key trends
- Role-specific gaps: FY2/SHOs scored <60% in 5/6 conditions for management and documentation.
- Guideline awareness: Only 45% of juniors could correctly cite condition-specific NHS protocols.
- Escalation delays: 52% of FY2s deferred critical decisions to seniors, even with clear red flags.
Implications
These findings highlight systemic deficits in junior doctors’ preparedness for acute surgical emergencies, emphasising the need for standardised training in high-stakes decision-making and guideline adherence.
Discussion
The findings of this study highlight a significant confidence gap among junior doctors in managing acute orthopaedic emergencies, particularly in documentation and emergent management planning. These results align with existing literature that underscores the challenges early-career physicians face when confronted with high-stakes clinical scenarios17. The perceived lack of preparedness among junior trainees suggests a need for more structured and practical educational interventions to enhance their confidence and competence in acute surgical care.
Key findings and implications
1. Inadequate preparedness among junior doctors
A recurring theme in this study was the self-reported lack of confidence among junior doctors, especially those in the early stages of training. This finding is consistent with prior research indicating that many trainees feel ill-equipped to handle time-sensitive surgical emergencies due to limited hands-on exposure18.
The steep learning curve in surgical specialties, combined with the unpredictable nature of emergencies, exacerbates this issue. Without deliberate training strategies, junior doctors may struggle to make critical decisions under pressure, potentially compromising patient outcomes.
2. Deficiencies in documentation and emergent management planning
The study identified documentation and emergent management planning as persistent weaknesses. Poor documentation can lead to miscommunication among healthcare teams, delays in treatment, and increased medico-legal risks19,20.
Additionally, the absence of structured management plans suggests a gap in systematic training on clinical decision-making pathways. These findings emphasise the need for standardised protocols, agreed templates, and checklists to guide junior doctors in acute scenarios.
Recommendations for intervention
To address these gaps, alongside traditional training courses and orientation sessions, the following evidence-based strategies are proposed:
1. Interactive teaching sessions, incorporating simulation and video-assisted reflection (VAR) training
High-fidelity simulation, including immersive VR-based scenarios that mirror real-world trauma situations, has been shown to boost diagnostic confidence, technical performance, situational awareness, and team dynamics in emergency contexts.
Conducting regular simulation training on prevalent surgical emergencies, such as acute abdominal issues, trauma cases, and postoperative complications, helps strengthen both clinical competencies and non-technical skills (e.g., communication, leadership). The integration of structured debriefing sessions enhances learning by enabling reflective practice and performance analysis21-24.
2. Visual display of guidelines and policy posters (NICE and local trust protocols)
Many junior doctors reported uncertainty in following best practices during emergencies. The implementation of easily accessible, specialty-specific guidelines, such as quick-reference handbooks or digital decision-support tools, could mitigate this issue. Studies have shown that adherence to clinical guidelines improves patient outcomes and reduces variability in care. Hospitals should ensure these resources are regularly updated and integrated into clinical workflows25,26.
3. Standardised documentation templates, safety checklists, and easy-to-use diagnostic mnemonics
Given persistent gaps in documentation, implementing standardised templates for acute surgical presentations may enhance accuracy and completeness. Electronic medical record (EMR) systems with embedded prompts for key clinical details (e.g., time of symptom onset, vital signs, initial management) could minimise omissions and support continuity of care. Additionally, the use of memorable mnemonics, such as the novel 'SKIN-SAVE' for necrotising fasciitis, offers a practical method to both recall diagnostic features and document them comprehensively. These initiatives should be supported by targeted training sessions on effective documentation techniques27-30.
References
- Mohammed G, Younis Z, Amin J, et al. Enhancing Junior Doctors’ Preparedness and Satisfaction in Trauma and Orthopaedics: A Quality Improvement Project With the Development of a Comprehensive Guidebook. Cureus. 2024;16(9):e70061.
- Matthews-King A, et al. A qualitative analysis of junior doctors' journeys to preparedness in acute care. BMC Med Educ. 2020;20(1):1-9.
- Croft S, Kuhrt A, Mason S. Are today's junior doctors confident in managing patients with minor injury? Emerg Med J. 2006;23(11):867-8.
- Chau AMT, Xu LL, Pelzer NR, Gragnaniello C. Timing of Surgical Intervention in Cauda Equina Syndrome: A Systematic Critical Review. World Neurosurgery. 2014;81(3-4):640-50.
- Woodfield J, Hoeritzauer I, Jamjoom AAB, Pronin S, Srikandarajah N, Poon M, et al. Understanding cauda equina syndrome: protocol for a UK multicentre prospective observational cohort study. BMJ Open. 2018;8(12):e025230.
- Gilbert F, Schneemann C, Scholz CJ, Kickuth R, Meffert RH, Wildenauer R, et al. Clinical implications of fracture-associated vascular damage in extremity and pelvic trauma. BMC Musculoskelet Disord. 2018;19(1):404.
- Zhang J, Bradshaw F, Hussain I, Karamatzanis I, Duchniewicz M, Krkovic M. The Epidemiology of Lower Limb Fractures: A Major United Kingdom (UK) Trauma Centre Study. Cureus [Internet]. 2024 Mar 20 [cited 2025 May 29];
- British Orthopaedic Association. BOASt - Diagnosis & Management of Arterial Injuries Associated With Extremity Fractures and Dislocations. Available at: www.boa.ac.uk/resource/boast-6-pdf.html.
- Bodansky DMS, Begaj I, Evison F, Webber M, Woodman CB, Tucker ON. A 16‐year Longitudinal Cohort Study of Incidence and Bacteriology of Necrotising Fasciitis in England. World J Surg. 2020;44(8):2580-91.
- Hsiao CT, Chang CP, Huang TY, Chen YC, Fann WC. Correction: Prospective Validation of the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) Score for Necrotizing Fasciitis of the Extremities. PLoS One. 2022;17(6):e0270726.
- Torlincasi AM, Lopez RA, Waseem M. Acute Compartment Syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2025 May 30].
- McDaid D, Park AL, Gall A, Purcell M, Bacon M. Understanding and modelling the economic impact of spinal cord injuries in the United Kingdom. Spinal Cord. 2019;57(9):778-88.
- Recommendations | Spinal injury: assessment and initial management | Guidance | NICE [Internet]. NICE; 2016 [cited 2025 May 30].
- Mathews CJ, Weston VC, Jones A, Field M, Coakley G. Bacterial septic arthritis in adults. Lancet. 2010;375(9717):846-55.
- Rutherford AI, Subesinghe S, Bharucha T, Ibrahim F, Kleymann A, Galloway JB. A population study of the reported incidence of native joint septic arthritis in the United Kingdom between 1998 and 2013. Rheumatology (Oxford). 2016;55(12):2176-80.
- Alexandersson H, Dehlin M, Jin T. Increased Incidence and Clinical Features of Septic Arthritis in Patients Aged 80 Years and above: A Comparative Analysis with Younger Cohorts. Pathogens. 2024;13(10):891.
- Ochsmann EB, Zier U, Drexler H, Schmid K. Well prepared for work? Junior doctors’ self-assessment after medical education. BMC Medical Education. 2011;11(1):99.
- Burridge S, Shanmugalingam T, Nawrozzadeh F, Leedham-Green K, Sharif A. A qualitative analysis of junior doctors’ journeys to preparedness in acute care. BMC Medical Education. 2020;20(1):12.
- Braaf S, Riley R, Manias E. Failures in communication through documents and documentation across the perioperative pathway. J Clin Nurs. 2015;24(13-14):1874-84.
- Davis J, Shepheard J. Clinical documentation integrity: Its role in health data integrity, patient safety and quality outcomes and its impact on clinical coding and health information management. HIM J. 2024;53(2):53-60.
- Hanke LI, Vradelis L, Boedecker C, Griesinger J, Demare T, Lindemann NR, et al. Immersive virtual reality for interdisciplinary trauma management – initial evaluation of a training tool prototype. BMC Medical Education. 2024;24(1):769.
- Mühling T, Späth I, Backhaus J, Milke N, Oberdörfer S, Meining A, et al. Virtual reality in medical emergencies training: benefits, perceived stress, and learning success. Multimedia Systems. 2023;29(4):2239-52.
- Walls R, Nageswaran P, Cowell A, Sehgal T, White T, McVeigh J, et al. Virtual reality as an engaging and enjoyable method for delivering emergency clinical simulation training: a prospective, interventional study of medical undergraduates. BMC Medicine. 2024;22(1):222.
- Heldring S, Jirwe M, Wihlborg J, Berg L, Lindström V. Using High-Fidelity Virtual Reality for Mass-Casualty Incident Training by First Responders - A Systematic Review of the Literature. Prehosp Disaster Med. 2024;39(1):94-105.
- Yoong SL, Hall A, Stacey F, Grady A, Sutherland R, Wyse R, et al. Nudge strategies to improve healthcare providers’ implementation of evidence-based guidelines, policies and practices: a systematic review of trials included within Cochrane systematic reviews. Implementation Science. 2020;15(1):50.
- Cheung A, Weir M, Mayhew A, Kozloff N, Brown K, Grimshaw J. Overview of systematic reviews of the effectiveness of reminders in improving healthcare professional behavior. Systematic Reviews. 2012;1(1):36.
- Ebbers T, Kool RB, Smeele LE, Dirven R, den Besten CA, Karssemakers LHE, et al. The Impact of Structured and Standardized Documentation on Documentation Quality; a Multicenter, Retrospective Study. J Med Syst. 2022;46(7):46.
- Bergs J, Hellings J, Cleemput I, Zurel Ö, De Troyer V, Van Hiel M, et al. Systematic review and meta-analysis of the effect of the World Health Organization surgical safety checklist on postoperative complications. Br J Surg. 2014;101(3):150-8.
- Tsai CH, Eghdam A, Davoody N, Wright G, Flowerday S, Koch S. Effects of Electronic Health Record Implementation and Barriers to Adoption and Use: A Scoping Review and Qualitative Analysis of the Content. Life (Basel). 2020;10(12):327.
- Wong CH, Khin LW, Heng KS, Tan KC, Low CO. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004;32(7):1535-41.