Intra-operative breakage of instrumentation during orthopaedic surgery
Authors: Shyam Kumar and Simon Britten
Intra-operative breakage of instrumentation during orthopaedic surgery
Contemporary trauma and orthopaedic surgery techniques involve the use of robust tools such as drills, reamers, hammers and chisels, alongside less durable instruments such as guidewires and Kirschner wires, used either to place cannulated screws, to guide reaming of the intramedullary canal, or to fix fracture fragments, either temporarily or definitively.
Given the light manual nature of orthopaedic procedures, it is inevitable, despite maximal care and good surgical technique, that occasional breakage of instrumentation may occur in the operating theatre. The majority of breakages tend to be drill bits or wires, with breakage occurring during fracture fixation. When breakage does occur, orthopaedic surgeons accept in broad terms that there is a balance to be considered – the risk of leaving the broken instrumentation in situ, weighed against the potential risks of attempted removal. Such considerations may be guided by whether the broken metal is deeply embedded in bone or protruding, the anatomical site of surgery including any adjacent neurovascular structures or joint surfaces, the nature of the retained metal – smooth K-wires and guidewires may have a propensity to migration, and the estimated additional surgical damage and risk of iatrogenic fracture if an embedded fragment of metal were to be pursued. Of lesser concern is the old adage ‘nobody ever looks good removing metalwork’. Consideration must also be given to the additional surgical time in light of any anaesthetic concerns, and also the fact that subsequent bone healing and callus formation may render later removal even more difficult. There is a relative paucity of studies on this topic, and to our knowledge no specific guidance exists from professional bodies in the UK and Ireland.
Consideration of the literature
A study involving 12,601 cases, (Haberal et al. 2021)1 reported that the breakage of an orthopaedic instrument occurred in 0.28% of procedures, with a rate of 0.64% in fracture fixation procedures and 0.08% in elective orthopaedic surgery. Overall the rate of instrument breakage was 7.44 times higher in trauma cases than in elective surgery cases (p = 0.001). In their study, the broken instrument was a K-wire in 16 (44.4%) cases, a screw in 14 (38.9%), and a drill bit in six (16.6%). They found that retained broken instrumentation tended not to have long term adverse health effects or patient outcomes. The commonest wire to break in this study was the guide pin for cannulated screws. As a recent study, the trend towards cannulated screw guide pins may reflect increased usage of cannulated screw systems over time.
An older prospective multi-centre study found the incidence of instrument breakage to be 0.35% (Pichler et al. 2008)2. Of note, the authors could not find any significant correlation between the surgeons’ experience and the rate of instrument breakage. Among the 42 cases of instrument breakage, 36 of them were buried safely in bone and none of these patients had any symptoms during the follow-up period. Loose drill bits and K wires were removed, as were wires lying in a joint. Given the absence of symptoms from metal buried deeply in bone, the authors concluded that removal of broken drill bits was not routinely indicated if securely embedded in the bone and is distant from blood vessels or nerves. They recommended removal of broken drill bits when loose, if both cortices of the bone are penetrated, there is proximity to a vessel or nerve, or if it lies in or near a joint. They recommended removal of smooth K wires given their known tendency to migrate.
Another two-year study looked at 7,775 procedures (Price et al. 2002)3. They found an instrument breakage rate of 0.18% of mixed trauma and elective cases (0.79% of trauma cases and 0.03% for elective cases). 11/14 breakages were broken drill bits. In seven cases the broken bit was left in situ. They noticed a higher incidence of breakages during fixation of fractures of the distal humerus.
The authors concluded that overall any persisting harm to patients was negligible in such cases. However, they emphasised that when such instrumentation breakage occurred, there was scope for improvement in both documentation and the explanation (if any) given to the patient. In contradistinction to Pichler et al’s study above, Price found that of the 14 breakages identified in 12 cases, only one case had a consultant as lead surgeon, with 8/12 where the lead surgeon was a less experienced Specialist Registrar.
Continuing the theme of drill bits in particular breaking, another two-year study of 8,132 patients, demonstrated a total of 30 (0.36%) cases of intra-operative instrument breakage, of which the majority were drill bits (Dharmshaktu et al. 2020)4. Hirt et al.5 reported a frequency of three drill bit failures per 1,000 internal fixations (0.3 %). They found the highest incidence during fixation of proximal femur fractures. The authors advised that a broken drill bit which is not in contact with an implant can be left in the body without any risk of delayed recovery. They recommended removal if the drill fragment is situated near a joint or if it can be easily removed without further trauma to the bone. They also suggest that once the fracture has healed the broken drill bit should be removed along with the implant provided no exceptional difficulties are involved. Migration of drill bits have been reported after fixation of acetabular fracture (Jamot et al. 2011)6. Broken wires or drill bits around the hip or pelvic cavity require particular attention and removal due to the risk of migration into the pelvis (Garabadi and O’Brien 2021)7. It remains to be seen whether the introduction of newer fixed angle locking plates have any effect on the incidence of drill bit breakage reported in the literature.
Even in some cases where the instrumentation has not broken, previously clavicle fracture fixation with K wires gave rise for concern regarding the uncanny ability of the wires to migrate – for example to the spinal cord (Fransen et al. 2007)8, to the oesophagus and brachiocephalic artery (Wada S, Noguchi T, Hashimoto T et al. 2005)9, to the lungs (Hegemann et al. 2005)10, and to the ascending aorta (Nordback I, Markkula H 1985)11. These reports are thankfully of historical interest only with the advent of improved surgical techniques for clavicle fracture fixation, but emphasise the need to be wary of migration of wires – both intact and broken – at certain anatomical sites.
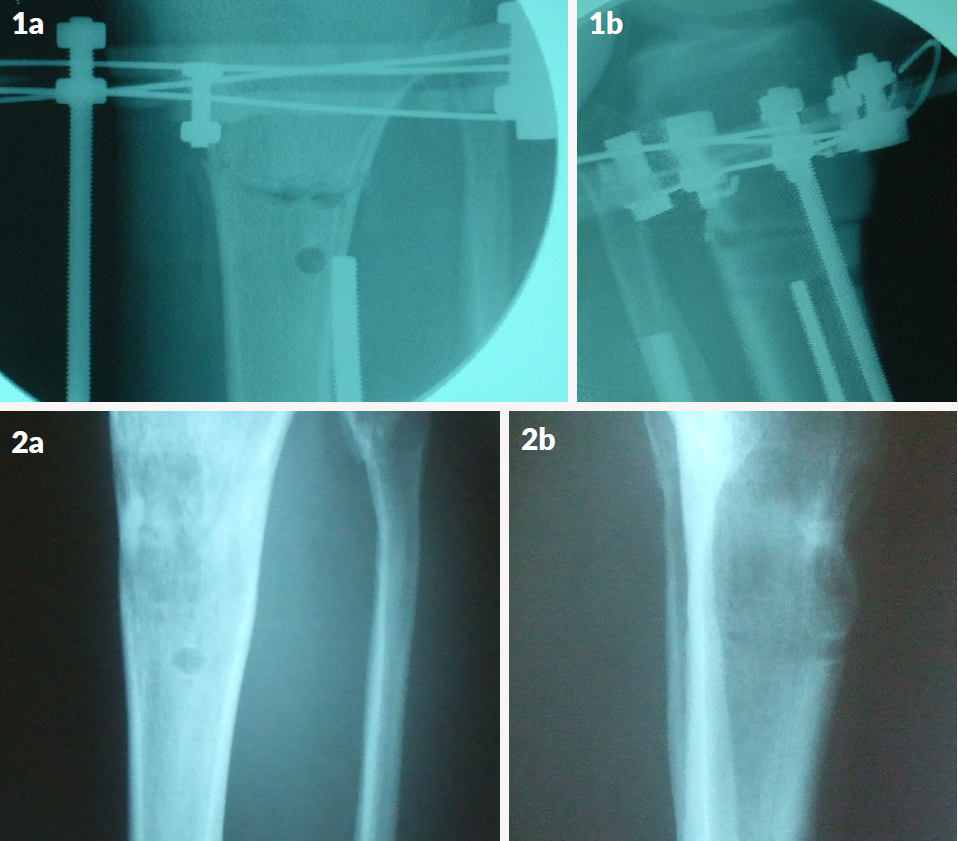
Images 2a and 2b at 19 months, prior to discharge show a more proximal column of regenerate bone which has healed and recorticated satisfactorily. More distally the circular defect in the anterior tibial cortex persists, but the rest of the cylindrical overdrilling track in the intramedullary bone has filled in and healed.
Medico-legal considerations
From the literature available, the average rate of breakage of a drill bit or wire during trauma and orthopaedic surgery is in the region of 0.3%. The rate of breakage is higher in trauma than elective surgery. Authors tend to agree that broken instrumentation which is well embedded and fixed in bone is unlikely to cause any problems and can be left in situ. Broken instrumentation particularly in the clavicle or pelvis may require removal due to risk of migration and subsequent injury to neurovascular structures. The same applies to loose metal threatening other adjacent structures, including the articular surface of a joint.
Intra-operative breakage of instrumentation should be explained as a material risk during the consent process for surgery. It should be explained that well seated and embedded broken drill bits and wires can be left in situ without retrieval, with no significant adverse consequences.
In the event of an intra-operative instrumentation breakage, appropriate documentation should be made in the operation note, including the weighing up process considering factors in play both for and against broken metal retrieval. The patient should be fully informed as soon as is practicable to do so, ideally when no longer under the effects of the general anaesthetic.
It should go without saying that good surgical technique must be employed at all times to minimise the risk of breakage of instrumentation, and the operating surgeon should be well versed in the techniques of broken metalwork removal, including but not limited to use of the broken screw removal set. Knowledge of case reports of other available novel techniques described to remove broken instrumentation may also be of use, for example Lim JW, McMillan TE, Stevenson IM 202112.
From a governance perspective, when formulating local policies, broken orthopaedic instrumentation identified intra-operatively and intentionally left in situ, should be clearly differentiated from inadvertent retained surgical instruments left in body cavities.
References
- Haberal B, Beyaz S, Effects of orthopaedic instruments breakage during surgery: A minimum five-year follow-up. Ann Clin Anal Med. 2021;12(4):443-6.
- Pichler W, Mazzurana P, Clement H, Grechenig S, Mauschitz R, Grechenig W. Frequency of instrument breakage during orthopaedic procedures and its effects on patients. J Bone Joint Surg Am. 2008;90(12):2652-4.
- Price MV, Molloy S, Solan MC, Sutton A, Ricketts DM. The rate of instrument breakage during orthopaedic procedures. Int Orthop. 2002;26(3):185-7.
- Dharmshaktu GS, Adhikari N, Mourya P, Bhandari SS, Singh P. Intraoperative instrument breakage during the orthopedic elective procedures: A retrospective single-center experience. J Orthop Spine. 2020;8:80-5.
- Hirt U, Auer JA, Perren SM. Drill bit failure without implant involvement — an intraoperative complication in orthopaedic surgery. Injury. 1992;23(Suppl 2):S5-S16.
- Jamot S, Razif A, Azhar MM, Abbas AA. Migration of a Broken Drill Bit After Acetabular Fracture Fixation. A Case Report. Malaysian Orthopaedic Journal 2011;5(1):56-9.
- Garabadi M, O'Brien S. Broken guidewire retrieval from the hip joint: A case report. Trauma Case Rep. 2021:35:100512.
- Fransen P, Bourgeois S, Rommens J. Kirschner wire migration causing spinal cord injury one year after internal fixation of a clavicle fracture. Acta Orthopædica Belgica. 2007;73:390-2.
- Wada S, Noguchi T, Hashimoto T, et al. Successful treatment of a patient with penetrating injury of the esophagus and brachiocephalic artery due to migration of Kirschner wires. Ann Thorac Cardiovasc Surg. 2005;11:313-5.
- Hegemann S, Kleining R, Schindler HG, Holthusen H. Kirschner wire migration in the contralateral lung after osteosynthesis of a clavicular fracture. Unfallchirurg. 2005;108:991-3
- Nordback I, Markkula H. Migration of Kirschner pin from clavicle into ascending aorta. Acta Chir Scand. 1985;151:177-9.
- Lim JW, McMillan TE, Stevenson IM. Broken guidewire intramedullary: what to do now? Ann R Coll Surg Engl. 2021;103(2):e56-e58.