Using a timeline chart table and game theory to improve operating theatre efficiency
By Conrad Lee and Charline Roslee
University Hospitals Dorset NHS Foundation Trust
Operating theatre efficiency is crucial for optimising patient outcomes, reducing waiting times, and maximising the use of resources. Despite the best efforts of surgical teams, inefficiencies often arise from various factors such as delays, miscommunication, and workflow disruptions. Most orthopaedic surgeons would have likely recalled feeling frustrated as they 'ran out of time' for the last operative case of the day, reluctantly resulting in case cancellation. To address these not-so-infrequent challenges, we explored the application of a reverse-timeline chart table incorporating the game theory to enhance operating theatre efficiency.
Game theory is a term used to describe the science behind strategic decision-making in social situations in which each participant can influence the outcome. Each participant has their own agenda they want to achieve but has to plan their best course of action based on the actions of others in any given situation. The strategic interaction between the participants can be modelled and mapped out mathematically using game theory principles to identify an optimal outcome for everyone involved in a given situation. There are many types of social scenarios 'games' which can be played, and each can be mapped out on theoretical models to help decipher the best strategies from each player. The game theory was originally developed for understanding economic behaviours (e.g. buying, selling) but can be applied to a wide variety of contexts, ranging from political decisions, biological evolution, to warfare strategies. An operating list is one such example of strategic social interactions where the game theory provides a framework for understanding the complex decision-making processes and strategic interactions between the participants.
To illustrate, we conceptualised the operating list as a 'cooperative' game in which the 'players' include the surgeons, anaesthetists, nursing and other healthcare staff. This cooperative game involves multiple decision-makers, each with their own interest. The game’s goal is to provide safe preoperative and operative patient care with the ultimate 'payoff' of completing all the cases on the list promptly without finishing late. The actions each individual makes could influence the outcome. By applying game theory to the operating list 'game', we can better understand the dynamics and strategically optimise the scheduling, resource allocation, and workflow processes to improve the overall efficiency. There are many different scenarios within the operating theatre environment that the different game theory strategies can be applied to1,2.
In our institution, we introduced a reverse-timeline chart table to support the application of game theory principles in the operating theatre. The reverse-timeline chart table (Figure 1 and Table 1) consists of a visual representation of the scheduled cases, with the finishing time of the list as the anchor point. The columns contain the key controllable milestones of the list, which include the send time, arrival to anaesthetic room time, the knife-to-skin time and out-of-theatre time. At the start of the day, the surgeon would fill out the chart working backwards from the finishing time, and allocate a target time for each specified milestone. Working backwards provides a focus on the completion of all the required cases whilst meeting the target timescale. By mapping out these milestones, the entire surgical team can visualise the anticipated timing in each subcomponent for each case and begin to identify and discuss any potential obstacles. The reverse-timeline chart also acts as a tool to empower each team member to communicate and be involved in strategic decision-making towards the common goal of timely completion of the operating list. In this cooperative game, each member may formulate their own strategies aligned to their expertise, experiences or personal interests.
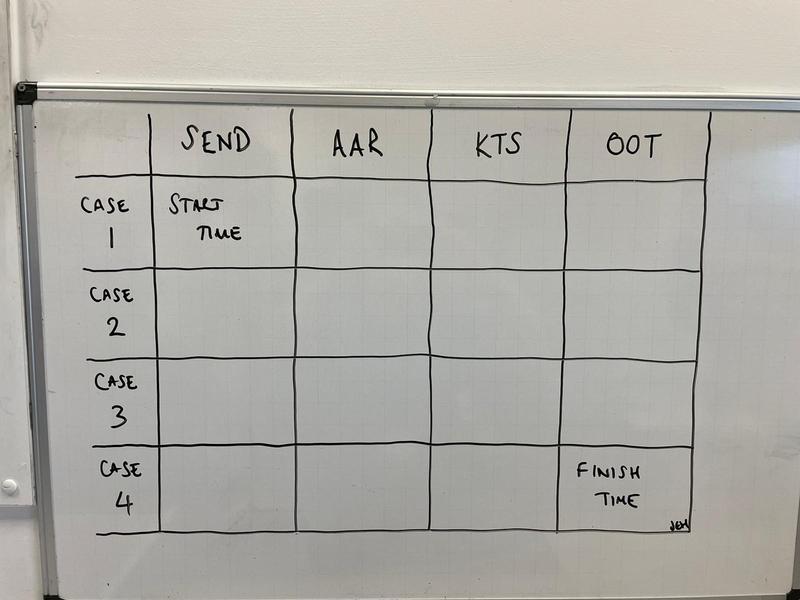
Figure 1: An example of the reverse time-line chart showing specific milestones (Send = time patient sent for, AAR = Time arrival to anaesthetic room, KTS = time of Knife To Skin, OOT = Time out of theatre)
|
|
Send |
AAR |
KTS |
OOT |
|
Case 1 |
08:40 |
09:00 |
09:30 |
11:00 |
|
Case 2 |
11:05 |
11:20 |
11:55 |
13:15 |
|
Case 3 |
14:00 |
14:15 |
14:30 |
15:30 |
|
Case 4 |
15:35 |
15:50 |
16:15 |
17:30 |
Table 1: An example of a completed reverse time-line chart. Note the time allocated between each milestones reflecting on the logistics of patient portering, anaesthetic preparations, actual surgical time as well as a lunch break. (Send = time patient sent for, AAR = Time arrival to anaesthetic room, KTS = time of Knife To Skin, OOT = Time out of theatre).
The reverse-timeline chart utilities the 'backward induction' strategy from game theory into optimising theatre efficiency. Without going into depths of the mathematics, the basis of backward induction is the process of identifying the optimal sequence of actions by reasoning from the endpoint back to its beginning within a dynamic game (one that evolves as the event plays out). As the day progresses, the team can monitor the actual progress against the planned timeline on the chart, and make real-time adjustments in their 'best response' strategies as needed. Each milestone is a nodal point where the team would decide their next actions depending on whether the milestone has been reached or not. For example, if one surgical case took longer than anticipated due to intraoperative complications, the team would have to decide the next 'best response' to the situation and strategise their next action. To make back time and avoid running behind schedule, the team could make proactive adjustments to the subsequent cases, such as performing concurrent preparation tasks (e.g. sending for the next patient early, preparing equipment in advance, staggering lunch breaks etc). On the other hand, if the team have no awareness of running behind, they may take on a passive approach and therefore take no action to compensate for the delay. The list is more likely to end up finishing late, or potentially result in case cancellations.
The application of this strategy however relies on rational behaviour and the active participation and collaboration between all members of the surgical team, assuming everyone actually wants to complete all the cases and finish on time. In reality, individual interests and lack of engagement may lead to suboptimal solutions or 'Nash equilibrium' scenarios where no one gains the optimal outcome. This is an example of the 'Prisoner dilemma' in which the players end up choosing a strategy that maximises their own payoff, but leads to a collectively suboptimal outcome. To illustrate this, imagine the above scenario where a case is running late due to unforeseen complications. Do the rest of the team pick to cooperate to work harder to make up for the delay, or do they simply take the passive approach knowing that they will finish early or on time at the expense of cancellation? If only part of the team takes on a proactive approach, there will be risk of overrunning. Without communicating their strategies and understanding the motivations of each team member, they will likely choose the passive approach, simply because the payoff seems better, (that is getting to finish work on time). This is illustrated in a 2x2 payoff table in Table 2. This is of course a simplified way to explain the social dynamics.
|
|
Theatre team |
||
|
Surgeon |
Proactive approach |
Passive approach |
|
|
Proactive approach |
Case gets done / team works harder |
Surgeon pushes on / risk of overrun |
|
|
Passive approach |
Theatre team pushes on / risk of overrun |
cancellation of case / team gets to go home early |
|
Table 2: A 'payoff' chart for the scenario where the operating list is running behind, illustrating the paradox of choosing the suboptimal approach (bottom right) for personal gain at the expense of case cancellation.
The important learning from the Prisoner dilemma is that individual actions based on self-interest will ultimately jeopardise the outcome as the group. Hence, trust, communication and cooperation are key components to overcoming the Prisoner dilemma, to achieve a strategically run operation list. The reverse timeline chart serves as a tool for open communication, in which the participants can cooperate and openly discuss their strategies to help reach the targets. The decision-making in this dynamic cooperative game requires flexibility and compromise.
Another key point to highlight from using the reverse timeline chart is that the team can, at the beginning of the day, negotiate the final deadline to send for the final case. This is particularly important because without formal communication and agreement, the personal agenda of finishing early or 'beating the traffic' may lead to early termination of the list. On the other hand, the 'let's wait and see' approach may lead to the final patient being starved unnecessarily even though it is clearly unrealistic to complete the final case on time. This also highlights the importance of understanding the personalities of the team. Being over-optimistic on the one hand may underestimate the timing required for each case, but being pessimistic means that theatre time is not fully utilised to its full potential. The team must therefore be critical and realistic about the estimated time they have set for their given task. It is beyond the scope of this article to dive into each type of 'game' within the game theory and its various strategies, but for theatre efficiency, we feel that the reverse timeline chart is a good tool to begin negotiations within the theatre environment. To adapt this to your own hospital, we recommend looking into the logistics and setup of your theatres, and then decide on your target milestones to use within the chart.
In conclusion, the application of game theory and the reverse-timeline chart table offers a promising approach to enhancing operating theatre efficiency. By treating the operating theatre environment as a cooperative game, we can better understand the strategic interactions and decision-making processes of the surgical team. The reverse-timeline chart provides a structured framework that emphasises the importance of backward planning, allowing the team to visualise and address potential obstacles proactively. This approach not only fosters better communication and collaboration but also enables real-time adjustments to keep the schedule on track.
References
- McFadden DW, Tsai M, Kadry B, Souba WW. Game theory: applications for surgeons and the operating room environment. Surgery. 2012;152(5):915-22.
- Marco AP. Game theoretic approaches to operating room management. Am Surg. 2002;68(5):454-62.