Charting the Progress – A summary of the BOA/BODS Survey
By Bob Handleya and Lara Bryanb
aConsultant T&O Surgeon, Oxford
bProject Manager, GIRFT Orthopaedic Trauma
Published 02 June 2020
BODS (British Orthopaedic Directors Society), as a group, provides an excellent source of opinion. Rejuvenated under the leadership of Julian Owen prior to COVID-19, weekly Zoom meetings – attended by over 80 Clinical Directors – have now cemented its activity and relevance.
Working in conjunction with Lara Bryan, the project manager for the GIRFT Orthopaedic Trauma Surgery work-stream (currently paused), an opportunity arose to undertake two surveys. In this article, I will present some of the findings of the second of these. The raw data without personal identifiers has already been made available to BOA members and GIRFT. If you are interested in having access to this data please contact [email protected].
Our second ‘COVID-19: T&O Situation Response Survey’ was conducted between 15th and 18th May 2020, using the online platform, Citizen Space. There were 76 responses from clinical directors, predominantly from Trusts in England. Many of the results are self-explanatory and so this article, in the main, is a series of illustrations. Additional information and explanation has been added where necessary.
In an attempt to estimate the burden on resources of conducting the same amount of Trauma work post-COVID as pre-COVID, two factors were taken into account: the extra duration of any procedure and the increased staffing levels required to run an individual theatre. The responses from the 76 CD’s were averaged and are expressed graphically in Figure 1. The results are compelling; on average, the Trauma operating that could be managed in a single theatre session pre-COVID, now requires 1.6 sessions. The increased staffing levels reflect both this increased number of theatre sessions and the extra staff per theatre. For surgeons this necessitates a 60% increase since a surgeon is required in each theatre even though it may be servicing fewer patients. No extra surgeons were needed per theatre and so the surgical resource therefore matches that of theatre lists. For each of the other staff groups there was a greater increase as on average there were more of each required for an individual list. The required number is therefore greater than the raw increase in theatre lists. For anaesthetists it was more than double. When scrub staff and anaesthetic assistants were combined, it revealed a figure of close to 2 extra staff required per theatre. As Figure 1 highlights, the net result shows that the number of scrub/anaesthetic assistants would need to increase by a ratio of 3:8 to manage the same amount of operative Trauma today. The stark conclusion being that if 30 scrub/anaesthetic assistant sessions were needed to service the patients on 10 old theatre lists to manage the same volume of patients currently, would take 80.
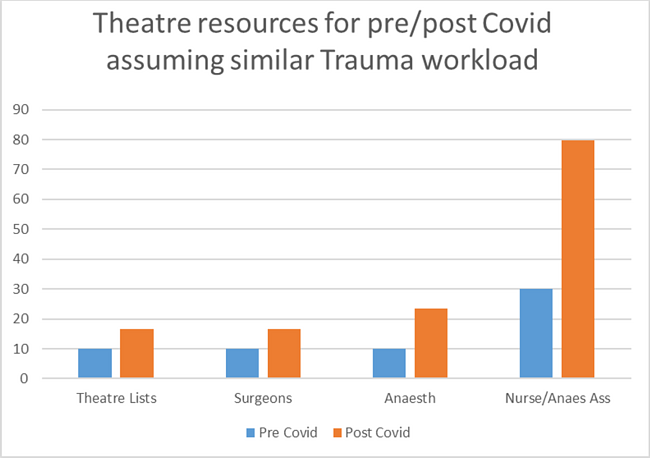
Figure 1
As elective work is not yet underway, respondents were asked to estimate the resources required for a similar question in relation to elective arthroplasty. Again, as indicated in Figure 2, the responses are very similar. This can be interpreted as the respondents anticipating that scheduled work – like Trauma – will also take longer and require additional staff. This highlights the need to establish working practices that allow a rate of theatre throughput much closer to pre-COVID levels. Without this adjustment, the number of cases that can be treated will presumably be severely limited by available resources.
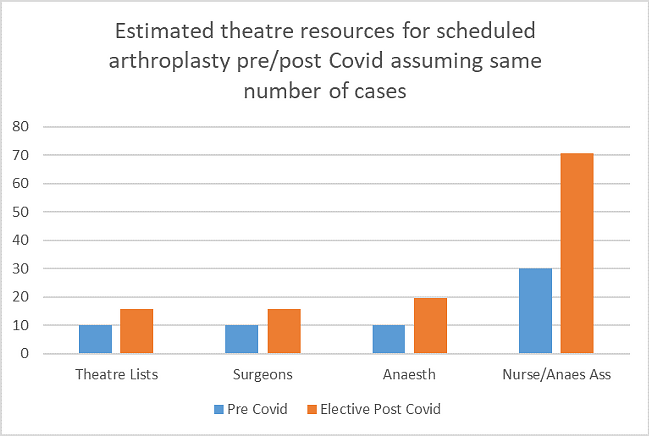
Figure 2
PPE has been a source of much discussion. It was identified as being a limited resource by about 10% of Trusts and the components in short supply were variable, as shown in Figures 3 & 4. The supply chain for PPE will no doubt be stressed more as there is a resumption of work in a wide range of occupations where it will be required. There will remain a need for vigilance to avoid those areas of greatest urgency being compromised.
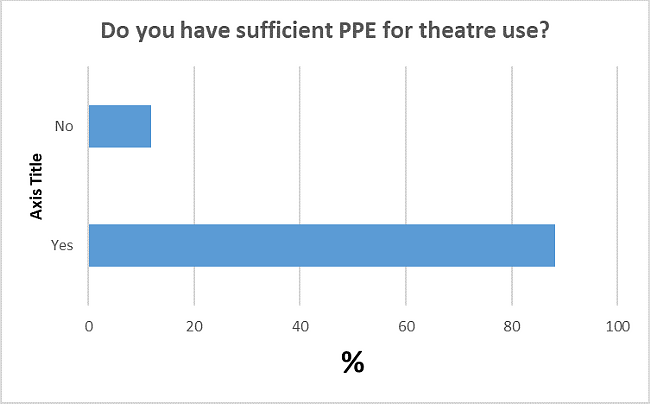
Figure 3
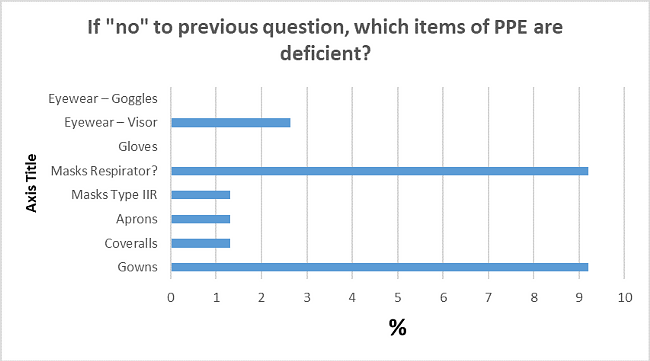
Figure 4
A number of questions relating to the resumption of ‘normal’ work were asked and are represented in the figures 5-10, below.
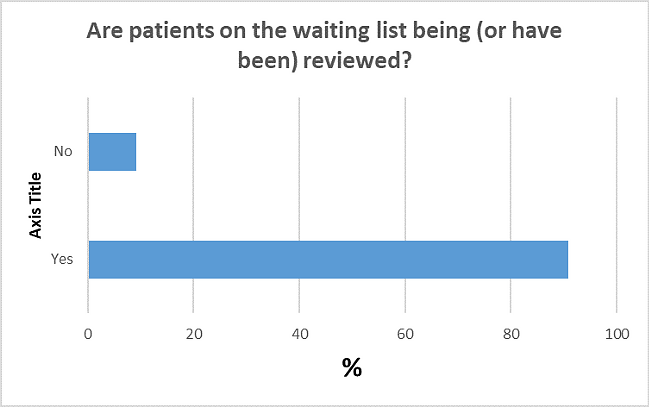
Figure 5
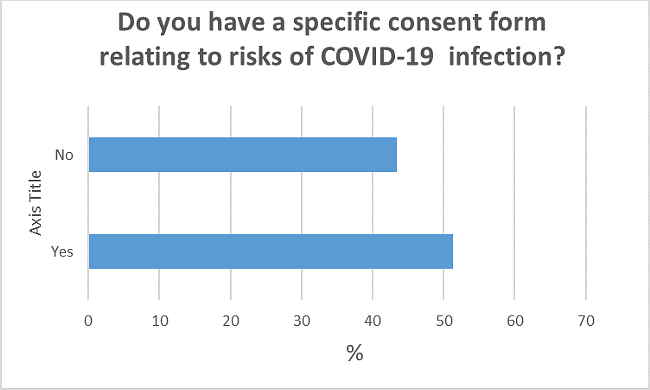
Figure 6
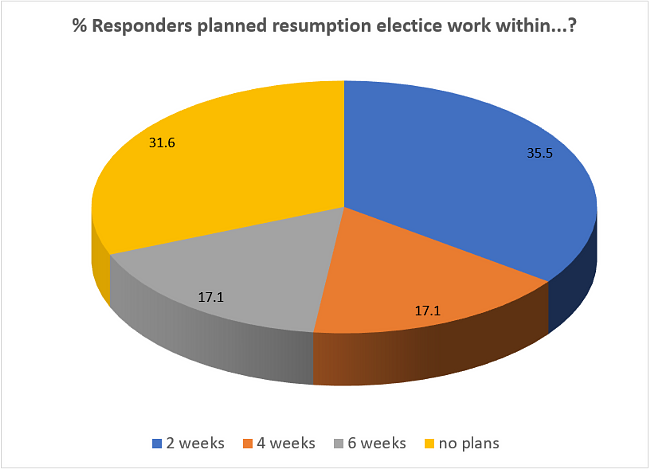
Figure 7
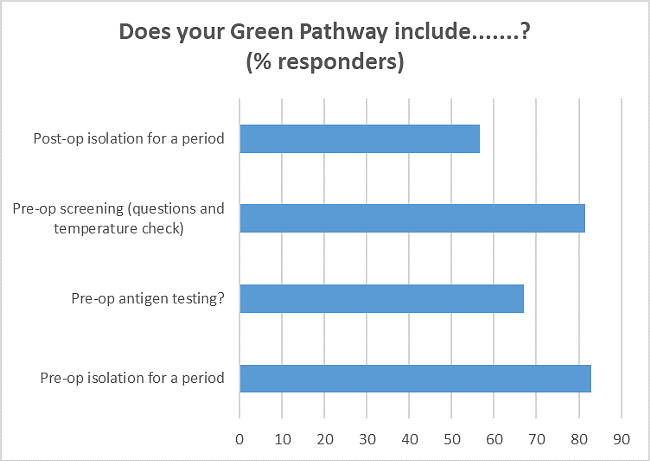
Figure 8
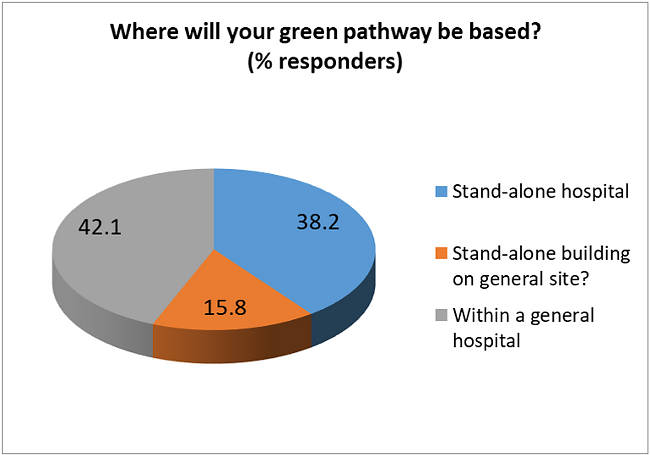
Figure 9
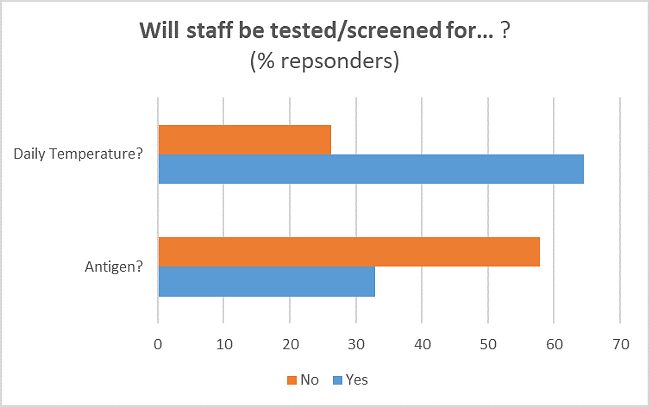
Figure 10
As can be seen from the previous figures there is a significant variation in practice and approach to the resumption of scheduled work. Indeed just a few weeks ago there was general expectation that central guidance would be issued in this regard. As can be seen in Figure 11, the majority of respondents considered any official guidance, issued to date, to have been insufficient. It was asked what specific guidance was desired; there was a range of free text answers. The responses can be seen on the comprehensive response spreadsheet by requesting access from [email protected]. These are in the main predictable and I suspect could have been predicted centrally and addressed, but clearly a decision was made not to.
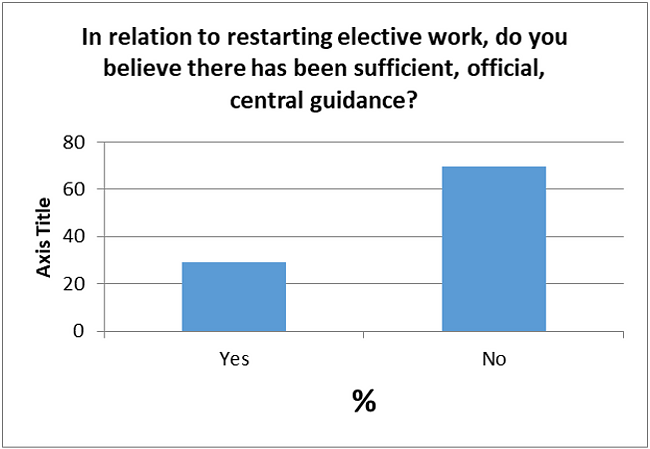
Figure 11
The final question related to collaboration. A key objective of GIRFT and espoused by Professor Tim Briggs in the resumption of scheduled work, is the opportunity to work with other units to achieve better results. Figure 12 shows that more than half of all CDs who responded to this question confirmed that the opportunity to work with neighbouring trusts had not yet been taken.
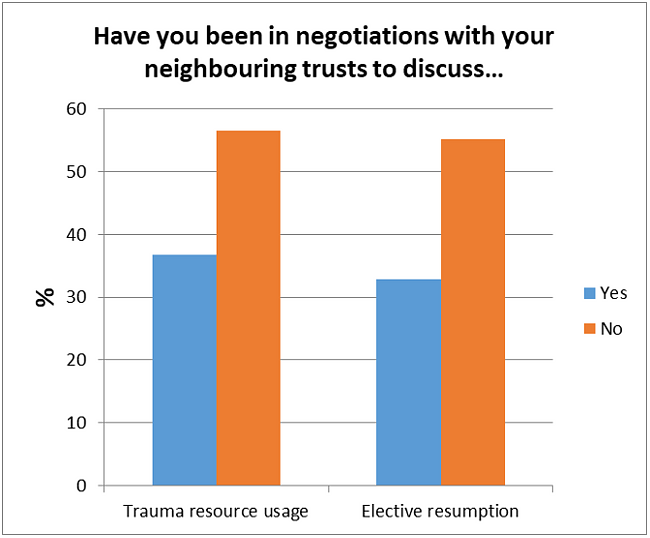
Figure 12
Summary
The BODS forum is a valuable source of informed opinion. The information in this survey has already been fed back centrally. We aim to use this group to get further insights into the current practice and intentions of our colleagues. The responses in this survey were predominantly from English Trusts, the net has now been spread wider to better reflect the ‘B’ in the BOA and BODS.
The absence of central guidance is noted and regretted by the majority. Without it, there is variation in the approach to the resumption of ‘normal’ work. Networking is therefore likely to be of greater importance as we aim to share the best practice of others.
Finally, what I take from the survey results on theatre resource is that there is the potential for our future work to be severely limited by lack of that resource. We need to evolve our working practices to get back closer to a near normal pace of operating and standard staffing levels. Should we not manage to do this we will risk being squeezed in the tussle for the resources of theatre space and skilled staff by ‘urgent work’.