Commonly missed injuries in the foot and ankle
Author: Patrick Laing
Commonly missed injuries in the foot and ankle
Patrick Laing is a Consultant Orthopaedic foot and ankle surgeon. He trained in London, Australia and Liverpool before taking up a Consultant post at the Wrexham Maelor and the Robert Jones and Agnes Hunt Orthopaedic Hospital in Oswestry in 1994. He is a Past President of the British Orthopaedic Foot and Ankle Society and past Council Member and Membership Secretary of the European Foot and Ankle Society. He is retired from NHS practice but is still involved in clinical research and teaching.
The foot and ankle are a complex unit comprising 26 bones and 33 joints. Many of the joints and structures require multiple views to fully assess them and certain injuries are not infrequently missed. This article highlights a number of the more commonly missed injuries and how to avoid that but is not meant as an exhaustive review of each injury. The common theme is an awareness of the possibility of the injury combined with a careful history and examination of the patient. In a litigious society, missed diagnoses and delayed treatment are costly to the NHS and stressful for the clinician and the patient.
Lisfranc injuries: A Lisfranc injury is an injury of the tarsometatarsal joints. It is a relatively rare injury, <1% of all fractures, and can be initially missed, or misdiagnosed, in 20-40% of patients. The mechanism of injury will typically occur with axial load on a plantar flexed foot, usually combined with a twisting element. It was originally described in 1815 by Jacques Lisfranc, a Surgeon and gynaecologist in Napoleon’s army, who described an injury, and amputation, caused by a soldier falling from his horse with the foot caught in the stirrups. Lisfranc injuries can involve all the tarsometatarsal joints, just the 1st or one or more of the lesser metatarsals. High energy injuries, e.g. following an RTA, are easily diagnosed. It is the more subtle injuries occurring in sport, or after a low energy fall, which can be missed. The patient may feel a pop in their midfoot and present with midfoot pain on weight-bearing. One of the hallmarks of a Lisfranc injury is plantar midfoot bruising (figure 1). If one sees that then you should assume the diagnosis of a Lisfranc injury, unless proven otherwise. Examination will reveal pain and tenderness on palpation and movement of the tarsometatarsal joints. Passive abduction and pronation of the midfoot may elicit pain. The piano key test isolates movement of one metatarsal in dorsiflexion and plantar flexion, whilst steadying the rest of the midfoot, and may help to localise an injury. Standard DP, oblique and lateral X-rays should be taken and, if a Lisfranc injury is suspected, you should do bilateral weight-bearing X-rays, for comparison, if the patient can tolerate that.

Figure 1: Plantar bruising in acute Lisfranc injury.
The weight-bearing acts as a stress which can reveal an occult Lisfranc injury. On a normal weight-bearing X-ray the medial border of the 2nd metatarsal lines up with the medial border of the intermediate cuneiform. The base of the 2nd metatarsal is recessed between the medial cuneiform and 3rd metatarsal. It is held in place by three oblique ligaments between the medial cuneiform and 2nd metatarsal. The central interosseous Lisfranc ligament is the strongest, followed by the plantar ligament and the weaker dorsal ligament. There is no intermetatarsal ligament between the 1st and 2nd metatarsals. A normal DP X-ray shows alignment of medial border of the 2nd metatarsal with the medial border of the intermediate cuneiform. A normal oblique X-ray shows alignment of the medial border of the 4th metatarsal with the medial border of the cuboid. If either of these views shows subluxation of the metatarsal base, usually laterally, that indicates a Lisfranc injury (Figure 2). The key is usually the alignment of the base of the 2nd metatarsal and other indicators can be a fleck sign between the base of the 1st and 2nd metatarsal, indicating a bony avulsion (Figure 3), and diastasis between the 1st and 2nd metatarsal, the M1-M2 gap, of >2mm.

Figure 2: 2nd metatarsal base is subluxed laterally.

Figure 3: Fleck sign.
However, one needs to be aware that the 1st metatarsal base can be unstable and have drifted laterally. If the diagnosis is not certain then additional investigations can include MRI, CT scan and stress views under anaesthetic. An unstable Lisfranc injury requires stabilisation to restore the normal anatomy as incongruity is associated with a poor result. If a diagnosis of a midfoot sprain is made, that is a Lisfranc injury until proven otherwise. The literature is not definitive on how late you can reduce and stabilise a Lisfranc injury, but you can probably do this up to six weeks. If degenerative changes are already apparent, you are probably better to fuse the joints.
Anterior process of the calcaneum (APC): APC fractures have been considered rare injuries, <3% of extra-articular calcaneal fractures, but the true incidence is probably higher as many of these fractures are missed on initial presentation. It is estimated that up to 40% may be missed on presentation to A&E. The mechanism of injury is thought to be inversion of a plantar flexed ankle which causes the bifurcate ligament attachment to pull off the APC. Because the mechanism is similar they are misdiagnosed as an ankle sprain. These fractures can be classified as type 1 – undisplaced, type 2 – displaced but extra-articular and type 3 – displaced intra-articular. These injuries are often misdiagnosed as sprained ankles as the history will be an inversion injury. Careful examination will reveal tenderness over the APC rather than the lateral ligaments of the ankle but there may be both. AP and lateral X-rays of the ankle may show the fracture on the lateral view, but it can be hard to visualise. A medial oblique view will show the anterior process better. If a fracture is suspected but not confirmed then a CT scan will make the diagnosis and show the extent of the fracture. It may be incidentally picked up on MRI (Figure 4).
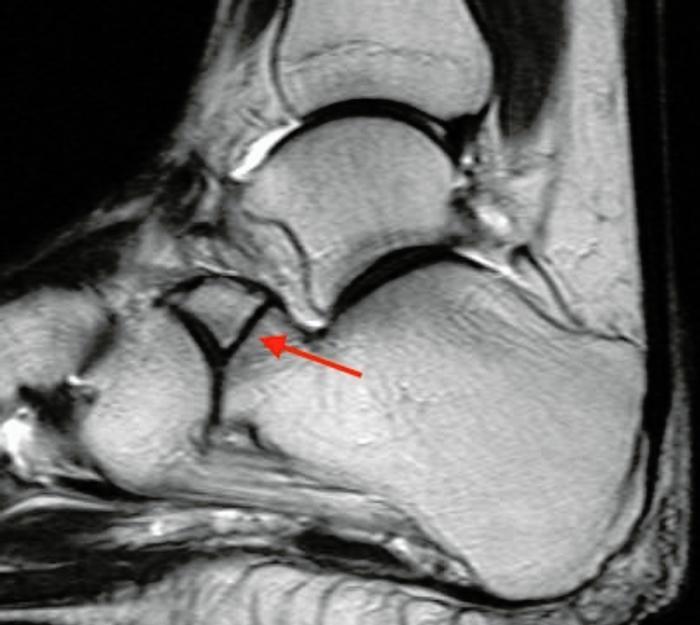
Figure 4: APC fracture involving calcaneo-cuboid joint diagnosed late.
Most of these fractures can be treated non-operatively. Treatment is not standardised but most treatment regimens advocate a period of immobilisation varying from plaster to a boot with protected weight-bearing for up to six weeks. The type 3 fractures involving the joint can be an indication for ORIF if the fragment is large enough. A number of these APC fractures may go on to non-union and cause ongoing symptoms and that becomes a medico-legal problem if the diagnosis has been initially missed. Late treatment is usually excision of the un-united anterior process but patients may still experience ongoing problems and can develop osteoarthritis of the calcaneo-cuboid joint.
Lateral process of the talus: This is known as the snowboarder’s fracture and is another of the fractures along the lateral border of the foot which may be misdiagnosed as an ankle sprain. It is thought that 40-50% of these fractures can be missed on initial presentation, as the lateral process is very close to the tip of the fibula and the lateral ligaments. The fracture is uncommon, comprising <1% of ankle injuries. The mechanism is thought to be dorsiflexion and inversion of the foot. Careful palpation of the lateral border of the foot will reveal tenderness over the lateral process. The fracture is difficult to diagnose on plain X-rays, because of overlapping bony structures, and an index of suspicion is necessary. A lateral view of the foot, AP mortise view of the ankle and a Broden’s view of the subtalar joint are the best views to show it. Sometimes the degree of pain and swelling may suggest an underlying injury, despite negative X-rays, and a CT is necessary (Figure 5).

Figure 5: CT showing fracture lateral process talus.
Treatment depends on the size of the fracture, whether it is displaced and whether it involves the joint. Displaced fractures involving the articular surface are best treated with internal fixation. Delayed diagnosis >2 weeks has been associated with poorer outcomes.
Sustentaculum tali: The sustentaculum tali is the antero-medial shelf of the calcaneum which provides structural support for the talus and includes the middle facet of the subtalar joint. The spring ligament, tibiocalcaneal and medial talocalcaneal ligaments attach to it and FHL runs in a groove under it. Isolated fractures of the sustentaculum tali are rare and are usually associated with a fall or high energy trauma, combined with a twisting movement. The patient may complain of medial hindfoot pain and have an antalgic gait. Examination will show tenderness 2-3cm below the medial malleolus.
Passive extension of the great toe may produce medial hindfoot pain, due to irritation of FHL, and subtalar joint movement will be painful and limited. They can be difficult fractures to see on standard views of the foot and are best seen on axial views of the calcaneum and then a CT scan (Figure 6 &7). It used to be thought these were extra-articular fractures which could be treated non-weight-bearing for six weeks and with early range of movement exercises, as the fractures are usually minimally displaced. It is now thought best to reduce and internally fix them. These fractures can also occur in conjunction with other trauma, such as a subtalar joint dislocation.

Figure 6: Lateral X-ray sustentaculum tali fracture.

Figure 7: CT showing sustentaculum tali fracture.
Stress fractures: A fatigue stress fracture is a fracture in normal bone caused by overuse. An insufficiency stress fracture is a fracture occurring in abnormal bone caused by normal stresses. The characteristic is these fractures occur without a specific history of trauma. In the foot they most commonly occur in the metatarsals, navicular, calcaneum and sesamoids. The mechanism is repetitive activity such as running, jumping and dancing. Female athletes with amenorrhea, decreased bone mineral density and a restricted diet are particularly at risk. The 2nd and 3rd metatarsals account for >80% of metatarsal stress fractures as these two rays are the stiffest. Most will occur at the head and neck junction but proximal fractures of the 2nd metatarsal are common in ballet dancers.
Stress fractures of the 5th metatarsal can occur with pes cavo-varus feet due to overload laterally. Patients will present with pain on activity and relieved on rest but becoming more persistent with time. The initial diagnosis is clinical as plain radiographs may not show any changes for a few weeks. Later X-rays then show a fracture and callus formation around the fracture site. Treatment of a metatarsal stress fracture is protected weight-bearing for a few weeks until symptoms settle. Stress fractures of the 5th metatarsal are a specific entity outside the scope of this article. Navicular stress fractures occur in sports players, such as athletes, rugby players and basketball players and also in ballet dancers. Patients will present with midfoot tenderness which may be poorly localised but worse on exercise. The almost pathognomonic sign is an area of maximal tenderness over the proximal dorsum of the navicular known as the N spot. Definitive diagnosis is often delayed for months due to the vague nature of the pain and the low sensitivity of plain X-rays in the earlier stages. If suspected, an MRI scan is most sensitive in detecting an early stress reaction. The initial treatment may depend on whether the diagnosis is a stress reaction or a complete fracture.
For a stress reaction or dorsal cortex fracture, non-operative treatment with six weeks non-weight-bearing in a plaster may settle down symptoms. In elite sportsmen and for complete fractures then internal fixation may be preferred. If the fracture goes on to non-union and collapse then secondary osteoarthritis will supervene. Calcaneal stress fractures present with a history of heel pain on weight-bearing and no history of trauma. They occur commonly in runners and present with heel pain worse on activity and may also be at night. Examination will reveal tenderness on squeezing the posterior calcaneum. They are misdiagnosed as plantar fasciitis, or Achilles tendinopathy, as the X-ray signs are subtle. X-rays, initially normal, will show a poorly defined sclerotic band through the superior aspect of the calcaneal tuberosity which is perpendicular to the trabecular lines (Figure 8).

Figure 8: X-ray showing diffuse sclerotic band of stress fracture calcaneum.
These fractures can also occur in the inferior calcaneum. If suspected, an MRI scan will provide the diagnosis. Treatment is usually non-operative with initial non-weight-bearing followed by protected weight-bearing until the symptoms settle. Stress fractures of the sesamoid bones under the 1st metatarsal head can occur, particularly in dancers going frequently en pointe and in athletes. Patients will present with an insidious onset of pain under the 1st mtp joint during and/or after athletic activities. Pain is relieved by rest. On examination there may be tenderness over the sesamoids accentuated by palpation and hyperextension of the joint. Radiology includes standard foot views along with skyline views of the sesamoids. MRI and CT scans will help differentiate sesamoiditis and bipartite sesamoids from a fracture. Initial treatment is usually non-operative but non-union can occur and require surgery.
Peroneal tendon dislocation: Peroneal tendon dislocation occurs with dorsiflexion and eversion of the foot coupled with contraction of the peroneal tendons. The patient may feel a pop with the dorsiflexion of the ankle. This is an injury to the superior peroneal retinaculum (SPR) which allows the peroneal tendons to sublux, or dislocate, anteriorly. It is a rare injury, occurring in about 0.5% of traumatic ankle injuries, and is most common in sports people. The patient will present with swelling, tenderness and pain over the lateral ankle. It is misdiagnosed as an ankle sprain so may be initially missed. Patients may then present late with a snapping sensation over the lateral ankle as the peroneal tendons flick over the lateral malleolus and back.
In an acute injury the SPR is stripped from the lateral malleolus. In a grade 1 injury the fibrocartilaginous ridge is intact and elevated with the SPR in a grade 2 injury. A grade 3 injury is a bony avulsion of the SPR and this produces a characteristic rim fracture of the distal fibula (Figure 9). An MRI scan will diagnose grades 1 and 2 and provide information on the state of the peroneal tendons and any concomitant pathology. Patients can be treated non-operatively, although this carries a higher risk of recurrent dislocation than operative treatment. Active sportsmen, elite athletes and a grade 3 bony avulsion injury are indications to consider surgery.

Figure 9: Rim fracture of distal fibula.
Ruptured Achilles tendon: Around 12,000 Achilles tendon ruptures a year occur in the UK and 75% are related to sport. The Achilles tendon has a degree of elasticity but macroscopically fails with strain levels >8%. When it fails, it fails catastrophically with interfibrillar shear failure as the intermolecular cross links fail and the collagen fibres slip past each other. Diagnosing a rupture is a straightforward clinical diagnosis, yet 20-25% are missed at initial presentation. The typical history is a middle aged weekend warrior who is playing sport and thinks somebody, or something, has struck them on the back of the calf.
A history of sudden, acute pain in the Achilles tendon without a direct injury is pathognomonic of an Achilles tendon rupture, until proven otherwise. The patient is unable to finish the game and will limp into A&E. A patient can perform a double stance heel raise test as they push off with their good leg. They are unable to perform a single stance heel raise test on the injured side. Lying prone on an examination couch with the feet clear of the bed end, the injured foot will hang more vertically than the uninjured side with tension in the Achilles tendon (Figure 10). On palpation a gap between the tendon ends may be felt, but not always. There will usually be tenderness over the site of the rupture and there may be some swelling. The Thompson, or Simmonds, tests are known as the calf squeeze test. With the patient lying prone and the feet clear of the bed, squeezing the calf doesn’t produce any plantar flexion of the foot. It is always necessary to compare both calves, especially if a patient presents late. Sometimes, one can get a small jog of movement which may fool an examiner who has not performed the full gamut of tests. If a history and clinical examination are competently performed, an Achilles tendon rupture should always be diagnosed. If there is any doubt, then an ultrasound examination can be requested and that will confirm the diagnosis.

Figure 10: Functional lengthening of Achilles tendon.
One should be very wary of diagnosing a partial rupture and, if you think that, it should be treated as a complete rupture pending a scan. Any functional lengthening means the tendon has fully ruptured and should be treated as such. The importance of making a correct early diagnosis is to ensure the Achilles tendon heals up in a position of correct tension. When the tendon ruptures the proximal muscles, gastrocnemius and soleus, will contract and pull the tendon ends apart. A rupture of the Achilles tendon will always heal up, but if it heals up in a lengthened position then the patient loses plantar flexion power when walking. They then complain of a lack of power of push off and aching in the calf when walking. The shortened muscle unit is pulling on a lengthened tendon and it is not possible to exert good power. Current UK treatment is usually either the SMART or LAMP non-operative protocols. Elite sports people may be treated operatively.
Suggestions for further reading
- Moracia-Ochagavia I, Rodriguez-Merchain E. Carlos. Lisfranc fracture-dislocations: current management. EFORT Open Reviews. 2019;4:430-44.
- Dhinsa BS, et al. Fractures of the anterior process of the calcaneum; a review and proposed treatment algorithm. Foot and Ankle Surgery. 2019;25:258-63.
- Majeed H, McBride DJ. Talar process fractures: an overview and update of the literature. EFORT Open Reviews. 2018;3:85-92.
- Mu H, Xiangyang X, Gang B. Isolated fractures of the sustentaculum tali: Injury characteristics and surgical technique for reduction management. J Foot Ankle Surg (Asia-Pacific). 2014;1(2):48-51.
- Rajivan R, Hind J, Shrestha S, Ashwood N. Delayed Diagnosis of Calcaneal Stress Fracture: A Case Report. Cureus. 2025;17(4):e83161.
- Shakked RJ, Walters EE, O’Malley MJ. Tarsal navicular stress fractures. Curr Rev Musculoskelet Med. 2017;10(1):122-30.
- van Dijk PA, Gianakos AL, Kerkhoffs GM, Kennedy JG. Return to sports and clinical outcomes in patients treated for peroneal tendon dislocation: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2016;24(4):1155-64.
- Zhou K, Song L, Zhang P, Wang C, Wang W. Surgical versus non-surgical methods for acute Achilles tendon rupture: a meta-analysis of randomised controlled trials. J Foot Ankle Surg. 2018;57(6):1191-9.