When AI gets it wrong: Medico-legal accountability in orthopaedics
Author: Gary Mundy
When AI gets it wrong: Medico-legal accountability in orthopaedics
Gary Mundy has been a Consultant Lower Limb surgeon in Northampton since 2010, with a practice in hip and knee surgery. He completed his medical training in Manchester in 1996. He acquired specialist accreditation in Trauma and Orthopaedics in 2008, undertaking higher surgical training in Nottingham. He completed a Master’s degree in Medical Law and Ethics in 2020. Further subspecialist fellowship training was undertaken at the Royal National Orthopaedic Hospital, Stanmore, London.
Artificial intelligence (AI) refers to computer systems capable of performing tasks that traditionally require human intelligence, including learning, reasoning, language processing and decision-making. Several interrelated branches of AI are particularly relevant to orthopaedic practice.
Machine learning (ML) systems identify patterns within data and improve performance without explicit task-specific programming. Deep Learning, a subset of ML, uses multi-layered neural networks to learn complex representations and is particularly suited to image analysis. Neural networks form the backbone of most deep learning applications. Natural language processing (NLP) enables computers to interpret and generate human language, allowing analysis of unstructured clinical text.
ML tools have been developed to detect fractures1, identify implants2 and estimate post-operative outcomes3. Deep learning systems can analyse MRI scans for early osteonecrosis4 or analyse full leg standing radiographs identifying leg axis parameters5. NLP techniques allow automated interrogation of operative notes and clinic letters, supporting audit, research and workflow efficiency6.
AI-enabled instruments, while remaining under human control, are increasingly incorporated into robotic-assisted surgery and patient-specific instrumentation. Robotic platforms in orthopaedics are now widely deployed, with reported benefits including improved implant positioning accuracy, customised surgical planning, reduced soft-tissue disruption and faster functional recovery7.
Limitations and risks of AI systems
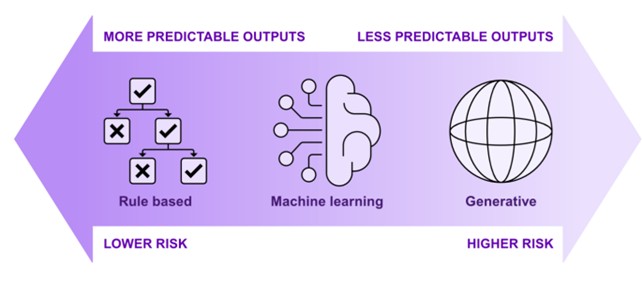
Despite its potential, AI carries significant and clinically relevant limitations that raise important medico-legal concerns. Clinicians should be aware that AI technologies incorporating ML and generative AI pose different risks to rules-based products8.
AI systems are only as reliable as the data on which they are trained. Incomplete, inaccurate or biased datasets may result in inequitable or unsafe clinical outcomes.
AI tools have disadvantaged certain patient groups due to underrepresentation in training data. High overall accuracy may mask poor predictive value for rare but clinically significant events known as the ‘accuracy paradox’. AI systems can exhibit a ‘black box’ problem, whereby the internal reasoning leading to a particular output is opaque.
When diagnostic or treatment recommendations cannot be meaningfully explained, clinicians may struggle to assess reliability or challenge erroneous outputs.
As AI systems are being deployed in more complex applications, there is an expanding need to value other important factors, such as safety, non-discrimination by the model, quantifying the uncertainty of model’s predictions, or the right to explanation of models’ results and features. This has led to the development of the field of explainable Artificial Intelligence (XAI). Additionally, European Union policy requires algorithms that make decisions based on user-level predictors and significantly affect individuals to provide an explanation on how they work9. Overfitting remains a further concern, where a model performs well on its training dataset but poorly when deployed in new clinical environments.
Ethical and medico-legal challenges
The increasing use of AI and robotic platforms raises complex ethical and legal questions for orthopaedic surgeons. Three illustrative scenarios highlight issues of medical device regulation, clinical negligence, informed consent and data protection.
Scenario 1: AI misdiagnosis
An AI system used in radiology fails to detect early lung cancer on CT imaging. The clinician relies solely on the AI output and does not independently review the scan. The cancer progresses to an incurable stage.
Scenario 2: Inadequate informed consent
A patient undergoes robotic-assisted surgery without being informed that a semi-autonomous AI system plays a substantial role in intra-operative decision-making. Post-operative complications arise, and the patient alleges they would not have consented had they known.
Scenario 3: Data misuse
An AI health application collects sensitive patient data but fails to adequately anonymise it. A subsequent data breach exposes identifiable medical information.
Medical device regulation
In the UK, most AI systems used for clinical purposes are regulated as medical devices under the UK Medical Devices Regulations 2002 (UK MDR)10. The definition of a medical device is intentionally broad and includes standalone software as well as software embedded within hardware. The Medicines and Medical Devices Act 2021 provides the statutory framework for post-Brexit reform of medical device regulations11. It enables amendment of the UK MDR to enhance patient safety, promote innovation and strengthen post-market surveillance. AI technologies are explicitly within scope of these reforms, reflecting concerns around algorithmic opacity, dataset bias and adaptive learning systems.
Devices are classified according to risk (Class I–III). Many AI applications in orthopaedics, particularly those influencing diagnosis, surgical planning or intra-operative decision-making, are likely to fall within higher-risk classes, requiring rigorous conformity assessment, clinical evidence and ongoing post-market surveillance.
At EU level, the Artificial Intelligence Act (2024) introduced a risk-based framework categorising AI systems as unacceptable, high, limited or minimal risk12. Most healthcare and surgical AI systems are designated high-risk, triggering stringent requirements relating to data governance, transparency, human oversight and monitoring, in addition to compliance with existing medical device regulations. UK-based developers supplying the EU market must therefore comply with this regime, indirectly shaping AI tools used within UK practice.
The UK Government’s AI Regulation White Paper (2023) adopted a pro-innovation approach based on five principles: safety, transparency, fairness, accountability and contestability13. Subsequent guidance published in 2024 is non-statutory and does not create binding legal obligations14. While this flexibility may encourage innovation, it risks regulatory fragmentation and uncertainty, leaving significant responsibility with regulators and industry.
Although attempts have been made to introduce AI-specific legislation, including the Artificial Intelligence Regulation Bill 2025, no statute currently provides comprehensive regulation of AI use in healthcare15.
Legal liability
Clinicians owe a duty of care to act in accordance with reasonable and accepted standards of practice. To establish negligence, a claimant must demonstrate breach of duty causing foreseeable harm. As AI systems become increasingly embedded in clinical decision-making, questions arise regarding the allocation of liability when harm occurs. Under English law, AI systems lack legal personality and cannot bear responsibility for harm. They are best understood as sophisticated clinical tools. Liability therefore rests with human actors: clinicians who rely on outputs, healthcare organisations that deploy systems, and potentially manufacturers where defects exist.
Uncritical reliance on AI outputs without appropriate clinical judgment is unlikely to satisfy the required standard of care. Conversely, software developers typically owe no direct duty of care to individual patients, although product liability or negligence claims may arise where known defects are ignored. The UK Jurisdiction Taskforce has recently consulted on liability for AI-related harm under English private law, highlighting the need for legal clarity as AI adoption accelerates16.
Informed consent
Patients have a legal right to make informed decisions about their care. Where AI systems materially influence diagnosis or treatment, this information may be material to consent and should be disclosed. You should explain why the AI tool is being used in the delivery of care, its benefits, limitations and risks. AI outputs should be reviewed and documented. In the context of robotic-assisted surgery, consent discussions should include the innovative nature of the procedure, the surgeon’s experience and learning curve, the role of AI or semi-autonomous systems, known and unknown risks associated with the technology, and available alternatives. AI outputs should be reviewed and documented. Failure to obtain valid informed consent may expose clinicians and institutions to liability, particularly in light of Montgomery17.
Data protection and privacy
AI systems in orthopaedics rely heavily on large datasets containing special category health data under UK GDPR and the Data Protection Act 201818. Data processing must be lawful, transparent and proportionate, with appropriate safeguards including anonymisation and security measures. Patients must be informed about how their data are used and retain rights of access, correction and erasure. Biased or incomplete datasets may also result in discriminatory outcomes, potentially engaging the Equality Act 201019.
Education and training
Safe implementation of AI and robotic systems requires structured service planning, workforce training and ongoing evaluation. National guidance, including GIRFT recommendations and guidance from the Royal College of Surgeons of England, emphasise governance, credentialing and outcome monitoring20. Without appropriate training and oversight, technological benefits may not translate into improved patient outcomes.
Conclusion
AI has the potential to transform orthopaedic practice, but it introduces novel ethical, ’legal’ and regulatory challenges. Existing frameworks are struggling to keep pace with rapid technological development, creating uncertainty around accountability, consent and safety. Surgeons must remain critically engaged, regulators must continue to adapt, and legal frameworks must evolve to protect patients while supporting responsible innovation.
Key learning points
- AI is already embedded in orthopaedic practice and its influence on clinical decision-making will continue to expand.
- In law, AI systems are treated as medical devices and clinical tools; responsibility for patient care remains with the clinician and provider organisation including documentation for outputs and decisions undertaken.
- Regulatory approval does not guarantee safety in every clinical context, particularly where data quality or bias exists.
- Patients should be informed when AI or robotic systems play a meaningful role in their diagnosis or treatment and why AI is being used in the delivery of their care.
- Safe adoption depends on governance, ’training’ and oversight as much as on the technology itself.
References
- Zheng Z, Ryu BY, Kim SE, Song DS, Kim SH, Park JW, Ro DH. Deep learning for automated hip fracture detection and classification : achieving superior accuracy. Bone Joint J. 2025;107-B(2):213-20.
- Karnuta JM, Murphy MP, Luu BC, Ryan MJ, Haeberle HS, Brown NM, et al. Artificial Intelligence for Automated Implant Identification in Total Hip Arthroplasty: A Multicenter External Validation Study Exceeding Two Million Plain Radiographs. J Arthroplasty. 2023;38(10):1998-2003.e1.
- Karlin EA, Lin CC, Meftah M, Slover JD, Schwarzkopf R. The Impact of Machine Learning on Total Joint Arthroplasty Patient Outcomes: A Systemic Review. J Arthroplasty. 2023;38(10):2085-95.
- Shen X, Luo J, Tang X, Chen B, Qin Y, Zhou Y, Xiao J. Deep Learning Approach for Diagnosing Early Osteonecrosis of the Femoral Head Based on Magnetic Resonance Imaging. J Arthroplasty. 2023;38(10):2044-50
- Salzmann M, Hassan Tarek H, Prill R, Becker R, Schreyer AG, Hable R, et al. Artificial intelligence-based assessment of leg axis parameters shows excellent agreement with human raters: A systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2025 Jan;33(1):177-90.
- Wyles CC, Fu S, Odum SL, Rowe T, Habet NA, Berry DJ, et al. External Validation of Natural Language Processing Algorithms to Extract Common Data Elements in THA Operative Notes. J Arthroplasty. 2023;38(10):2081-4.
- Robotic-assisted Surgery. A pathway to the future. Royal College of Surgeons of England. December 2025.
- AI Clinical Use Guide. Guidance for clinicians. Australian Commission on Safety and Quality in Health care 2025.
- Parliament and Council of the European Union, Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation). (2016). http://data.europa.eu/eli/reg/2016/679/oj.
- Medicines and Medical Devices Act 2021.
- UK Medical Devices Regulations 2002.
- European Union. Artificial Intelligence Act, 2024.
- Department for Science, Innovation and Technology. AI Regulation White Paper, 2023.
- Department for Science, Innovation and Technology. Initial guidance on implementing the UK AI regulatory principles, 2024.
- Artificial Intelligence (Regulation) Bill (HL) Private members bill 4th March 2025
- UK Jurisdiction Taskforce. Consultation on liability for AI-related harm, 2024.
- Montgomery v Lanarkshire Health Board [2015] UKSC 11.
- UK General Data Protection Regulation and Data Protection Act 2018.
- Equality Act 2010.
- Implementation of robotic assisted surgery (RAS) in England. GIRFT. July 2025.